
Bridging the Gap: A New Era in Canine Mitral Valve Repair with TEER
Myxomatous Mitral Valve Disease (MMVD) remains the most common cardiovascular pathology in dogs, accounting for roughly 75% of all canine heart cases. For decades, the veterinary community has balanced two extremes: palliative medical management, which eases symptoms but cannot stop structural decline, and open-heart surgery, which - while now getting quite sucessful - is limited by high costs, low geographical availability, and the intensive requirements of cardiopulmonary bypass.
The emergence of Transcatheter Edge-to-Edge Repair (TEER), specifically utilizing the V-Clamp device, holds the potential of provising a “middle ground.” This minimally invasive, beating-heart procedure offers a mechanical solution for patients who are not candidates for bypass or for owners seeking a (possibly) lower-risk or lower-cost alternative.
The Technology: How TEER Works
Adapted from the human MitraClip technology, TEER addresses mitral regurgitation by physically “clipping” the leaking valve leaflets together.
Steps Involved:
-
Beating-Heart Access: Unlike traditional surgery, TEER does not require stopping the heart. Surgeons perform a small (2-to-3-inch) incision (mini-thoracotomy) to access the heart apex. An introducer sheath is then passed directly into the beating left ventricle.
-
Precision Guidance: The procedure is performed under real-time 3D trans-oesophageal echocardiography (TEE/TOE) and fluoroscopy. This allows the interventionalist to precisely navigate the V-Clamp to the exact site of the leak typically the central A2 and P2 segments.
-
Creating a “Double Orifice”: By clamping the anterior and posterior leaflets together, the device creates a tissue bridge. This transforms the single leaking opening into two smaller, more competent orifices that allow blood to flow forward during diastole while sealing the “leak” during systole.
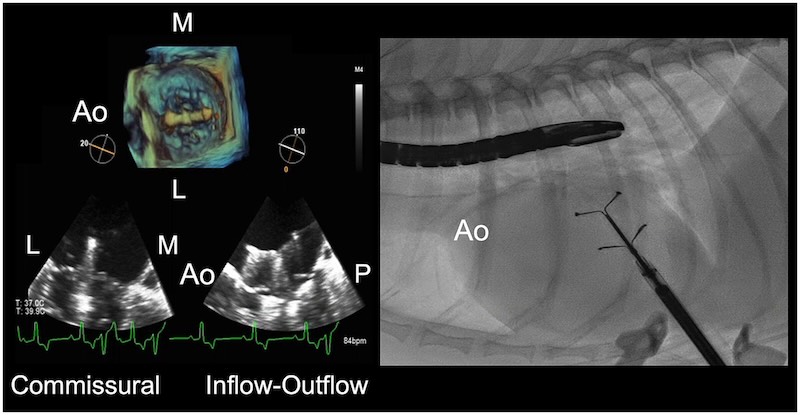
Image: TEER being guided by fluoroscopy and trans-oesophageal echo Potter et al (2024)
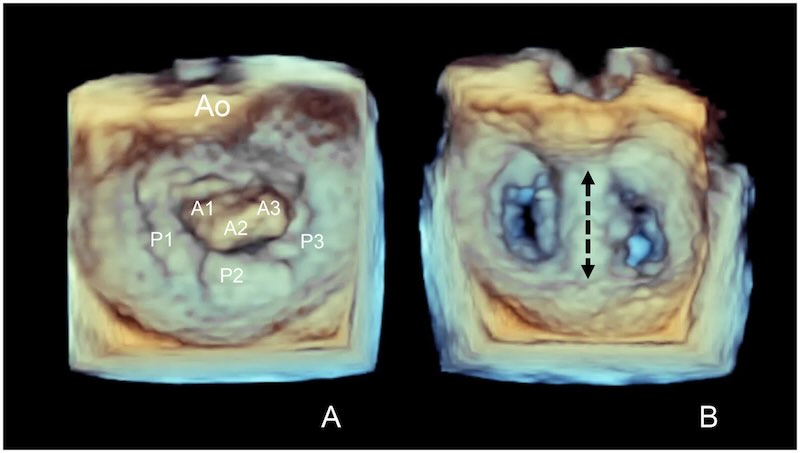
Image: Double Orifice valve Potter et al (2024)
The procedure requires quite a complex capture of the valve by the clamp device. Obviously this is a critical step, as a device that breaks free at this stage will cause likely fatal consequences. The ultrasound (colour doppler) can assess the success of the clamp location and be used to judge any fine tuning or even second clamp placement.
What is a V-clamp?
Edge to edge repair of a valve relies on a device clamping one edge of the valve to another, which seems counter intuitive but can dramatically improve the mechanical problem of valve deterioration. This makes a ‘bridge’ across the valve and clearly reduces the amount of flow orifice for forwards flow as well as reducing the backwards leak.
The V-clamp is made from a nickel-titanium shape-memory metal allow encased in a polymer, about 8mm in length. It is deployed from its sheath in a controlled way to allow careful contact with the dorsal and ventral surfaces of each anterior and posterior valve leaflets.
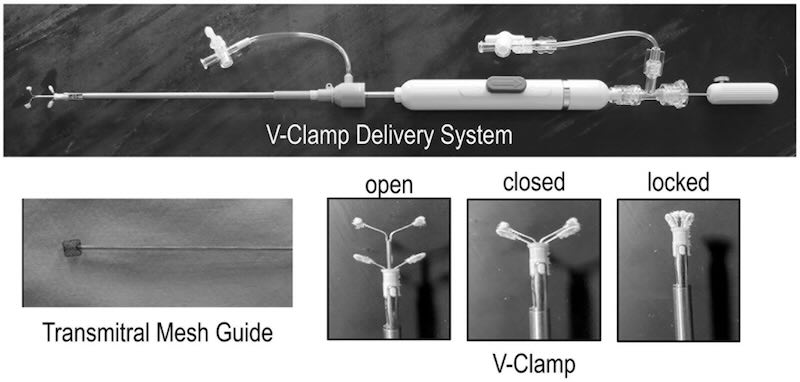
Image: V clamp device Potter et al (2024)
Patient Selection: Who is the “Ideal” V-Clamp Candidate?
Success with TEER is heavily dependent on rigorous patient selection. It is not a “rescue” procedure for end-stage failure, but rather a proactive intervention for stabilized patients.
Clinical Staging
The best candidates are dogs in ACVIM Stage B2 (heart enlargement but no symptoms) or early Stage C (congestive heart failure that has been stabilized with medication).
It is not usually advisable to undergo the risks of the procedure any earlier than this due to the current dangers of the procedure outweighing the benefits. A MINE-score of 7+ is usually advised.
Weight and Size
The procedure is optimized for small to medium breeds, typically between 3 kg and 15 kg. Although heart size is more crucial - in particular the annulus size of the mitral valve. Roughly the range that is possible with the current devices is 11mm to 23mm. But detailed discussion with your local surgical team is essential, and likely to need trans-oesophageal echo for final determination.
Anatomic Suitability
This is a complex area with rapidly changing ideas and research. For a low risk patient, the leak must be localized to the central portion of the valve (A2/P2). Dogs with leaks near the edges (commissures) or with excessively thickened or short leaflets may carry a higher risk of the device failing to “grasp” the tissue securely. Flail or billowing of the leaflet might increase risks of devices tearing the valve or dislodging. Again, detailed discussion with your local surgical team is essential.
Unsuitable patients
Typically some patients are not usually considered suitable. Again, advice from your local surgical team is essential:
- Those with atrial fibrillation
- Those with valve annulus diameters more than 23mm and less than 13mm.
- Those in Stage D heart failure (refractory)
- Those with significant co-morbidities, eg severe renal disease, or advanced neoplasia.
- Those with marked ‘flail’ (>45 degrees)
- Short leaflets (especially posterior leaflets <6mm)
- Very calcified or thickened leaflets
- Large ‘coaptation gap’ between the leaflets.
- Small ‘leaflet to annulus index’ (length of leaflet divided by annulus)
Clinical Outcomes: Life Beyond the Procedure
The data for TEER is highly encouraging compared to medical management alone. While open-heart surgery remains the “gold standard” for total valve reconstruction, TEER offers significant survival benefits.
-
Survival Rates: Approximately 80% of dogs with heart failure signs are still alive two years post-TEER, compared to a historical 15% survival rate for those on medication alone.
-
Rapid Recovery: Most patients are awake and walking within 24 hours of surgery and are discharged from the hospital within 1 to 3 days.
-
Reverse Remodeling: Successful repair often leads to the heart “shrinking” as the volume overload is reduced. This frequently allows for a significant reduction in the dosage of diuretics (heart failure medications).
| Metric | Medical Management | TEER (V-Clamp) | Open-Heart Surgery |
|---|---|---|---|
| Core Mechanism | Palliative medication to manage symptoms and delay heart failure. | Minimally invasive "clipping" of leaflets to create a double-orifice valve. | Definitive reconstruction of the valve using bypass (annuloplasty/chordae replacement). |
| Procedural Risk | Low; risks include kidney strain or electrolyte imbalances from diuretics. | Low to Moderate; ~95% survive to discharge. ~5% risk of major adverse events (e.g., detachment). | Moderate to High; ~90-95% survival. Risk associated with cardiopulmonary bypass and "stopping" the heart. |
| Patient Suitability | Appropriate for all MMVD stages, particularly early stages (A, B1) or end-stage palliative care. | Ideal for small/medium dogs (3-15kg) in Stage B2 or early C with focal central (A2/P2) leaks. | Best for complex valve anatomy (ruptured chordae, commissural leaks) or patients requiring definitive repair. |
| 2-Year Survival Rate | ~15% for dogs who have reached Stage C (congestive heart failure). | ~80% for stabilised patients post-procedure. | ~90%+ in high-volume, experienced surgical centers. |
| Quality of Life | Good while stable, but relapse is likely, requiring frequent medication adjustments. | Significant improvement; most dogs can reduce or even stop some heart failure medications. | Excellent; many dogs are able to discontinue all heart failure medications. |
| Estimated Cost (USD) | ~$100 per month for base medications like Pimobendan. | ~$16,000 - $20,000 including hospitalization. | ~$32,000 - $50,000 depending on complexity and location. |
| Global Treatment Centres | Universally available at almost all veterinary general practices. | Limited; ~20 specialised cardiac centers globally (e.g., USA, UK, EU, Asia-Pacific). | Extremely restricted; <10 centers worldwide (primarily UK, Japan, and very limited US/France). Very steep learning curve and need for multidisciplinary teams to be highly synchronised and experienced. |
Post-Operative Typical Advice
The transition from hospital to home is a critical period for TEER patients. While the procedure is minimally invasive, the first few weeks are essential for long-term success.
-
The 72-Hour Window: The most serious complication is device detachment, which occurs in roughly 5-7% of cases. The risk is highest in the first 48 to 72 hours while the heart tissue begins to grow over the clamp.
-
Resting Respiratory Rate (RRR): Owners are instructed to monitor their dog’s RRR while they sleep. A rate consistently below 30 breaths per minute is the goal. A sudden or steady increase above 30 bpm is often the first sign that the heart is struggling. This is recommended for all dogs in Stage B2 and Stage C regardless.
-
Strict Activity Restriction: For the first 14 days, dogs must be on “lead-only” activity for toilet breaks. No jumping on furniture, running, or rough play is allowed, as sudden spikes in blood pressure could stress the repair.
Complications
Clamp detatchment is of huge concern and will often cause a fatality. As this is a complex technique there is a huge learning curve, and as centres get more experience with the technique the incidence should drop. Rates of this are typically reported as 5-10%. But might be higher in centres that are relatively newer to the procedure.
In addition, thrombosis (clots) is reported, as is mitral valve stenosis and various rhythm abnormalities (such as atrial fibrillation and AIVR).
Red Flags for Immediate Evaluation
Owners and primary care vets should look for “red flags” that indicate a potential complication or recurrence of fluid in the lungs:
-
Persistent coughing, especially at night or after lying down.
-
Sudden weakness, fainting, or collapse.
-
Difficulty breathing or standing with an extended neck to catch their breath. Increased respiratory rate.
-
Refusal to eat or extreme lethargy.
Conclusion
TEER represents a paradigm shift in how we approach canine heart disease. By addressing the mechanical “leak” early in the disease process, we can offer pets a higher quality of life with fewer medications and more time with their families. For veterinary professionals, TEER is a powerful new referral option; for owners, it is a message of hope for their beloved companions.
Centres offering TEER
This list is a rough guide to current centres offering the procedure around the world. As the procedure is new and things are changing fast it is not exhaustive by any means. Some centres are currently utilising visiting teams from other centres:
USA
Colorado State University - highly experienced
Washington - Olympic Veterinary Cardiology
Florida - Sawgrass Veterinary Cardiology
Florida - Blue Skies Veterinary Cardiology
University of Minnesota
Texas A&M
University of Illinois
Europe
Munich - LMU Munich - highly experienced
Bristol - BVS
London - RVC London
Asia/Pacific
Brisbane - Veterinary Cardiologists Australia
Singapore - Atlas Vet
Japan - Azabu University
Korea Animal Medical Centre
Thailand - Chulalongkorn University
China - Xinyu Animal Hospital
References:
Potter BM, Orton EC, Scansen BA, Abbott-Johnson KM, Visser LC, Chi I-JB, Ross ES, Del Nero B, Tantisuwat L, Krause ET, Rezende ML and Mama K (2024) Clinical feasibility study of transcatheter edge-to-edge mitral valve repair in dogs with the canine V-Clamp device. Front. Vet. Sci. 11:1448828
Images from above article reproduced under CCBY licence.