
Echocardiography Basics 4: Why the Long-Axis Left Atrium (LAD) is Often Better
In our previous discussions, we explored the “gold standard” LA:Ao ratio. However, we also acknowledged the coal face realities: motion artifacts, pulmonary vein dropout, breed variations, and the difficulty of obtaining a perfect “Mercedes Benz” sign. In trying to use a simple aortic root measurement as a ‘constant’ to compare the LA to, we have ended up creating a very unreliable measurement that now has 2 possible sources of error. If you find yourself frustrated by the variability of the short-axis view, you are not alone.
Veterinary cardiology is increasingly moving toward the Left Atrial anteroposterior Dimension (LAD). Measured from the right parasternal long-axis view, the ‘4 Chamber’ view, this metric is often more repeatable, easier to acquire in a struggling patient, and provides a clearer picture of the atrium’s true expansion.
The View: Acquisition of the “Heart Homepage”
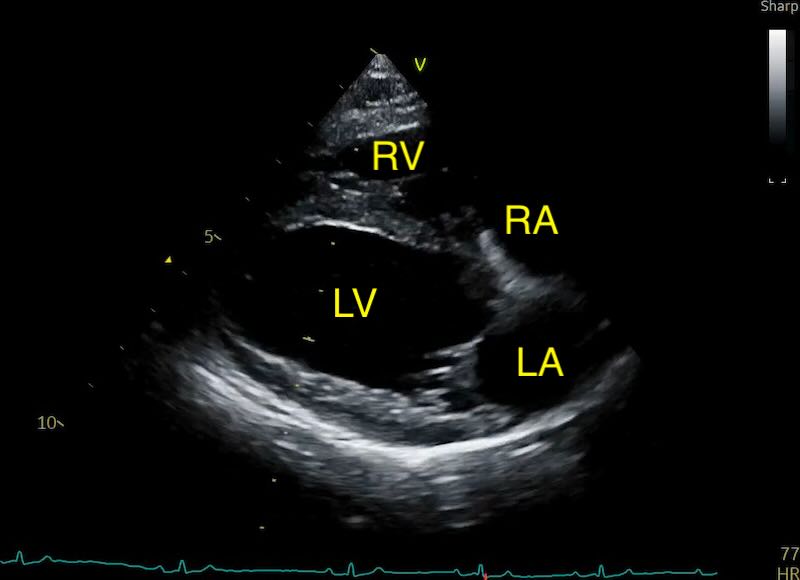
The LAD is measured using the Right Parasternal Long-Axis 4-Chamber view (RPLA4Ch). This is often called the “heart homepage” because it allows for a comprehensive subjective and objective assessment of all four chambers simultaneously. See our article on echo views here.
As a quick summary:
- Acquisition: With the dog in right lateral recumbency, place the probe at the point of the strongest apical beat. Align the probe parallel to the long axis of the heart, with the transducer mark (and your forefinger) pointed toward the dog’s head.

- Optimisation: Aim to maximise the length of the left ventricle, ensuring the apex is visible and the mitral valve is clearly defined. Avoid any aorta showing (5 chamber view).
Methodology and Timing
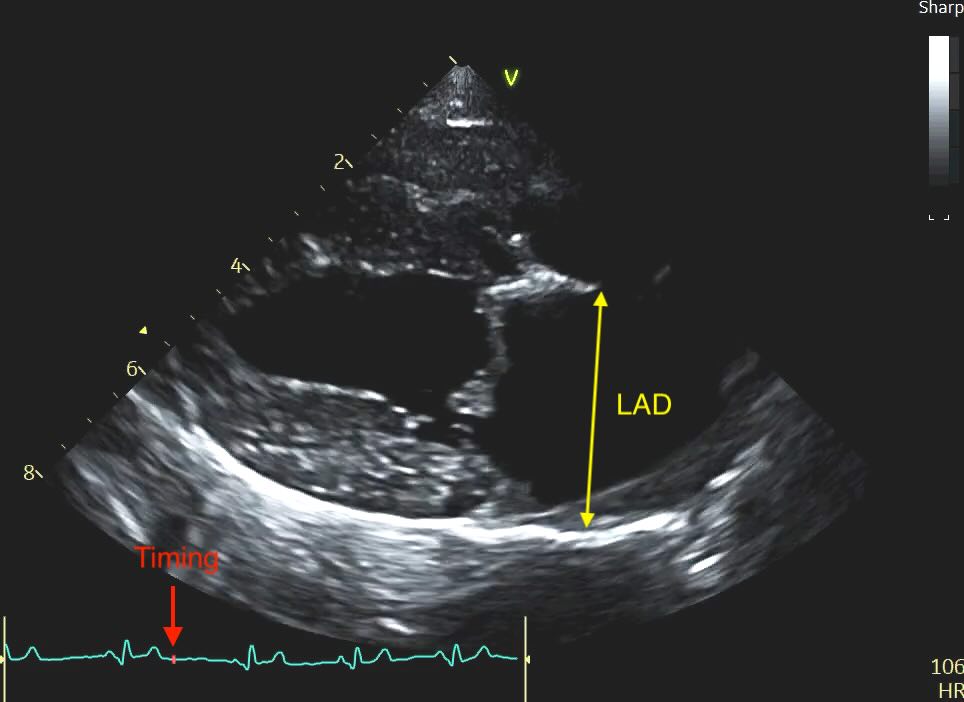
Unlike the LA:Ao, which we time to early diastole, the LAD is measured at end-systole. This is when the left atrium is at its maximal volume, having just finished filling from the pulmonary veins.
- The Timing: Select the frame just before the mitral valve opens (or 1-2 frames after the peak of the T-wave if using an ECG). This is easy with practice, scroll backwards in your loop until you have a closed valve, then step forward frame by frame until it pops open, and go back again 1 frame.
-
Caliper Placement:
-
Measure the distance from the inner wall (endocardial border) of the middle of the interatrial septum to the inner wall of the posterior free wall.
-
The line must be at the widest point of the atrium and must remain parallel to the mitral valve annulus.
-

The Problem of the “Bowed” Septum
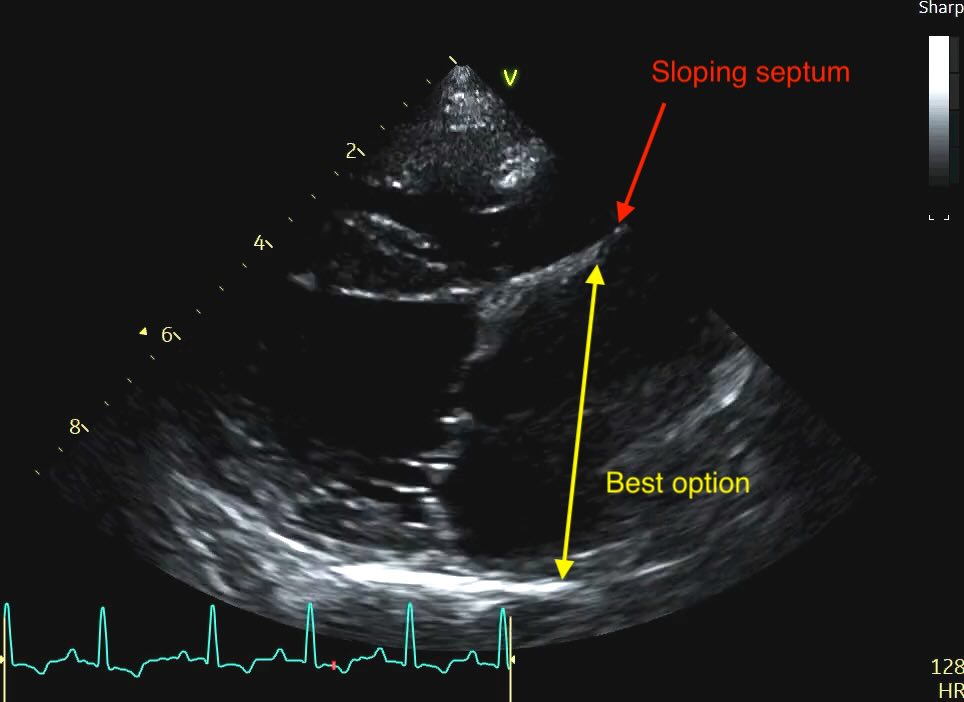
Sometimes you’ll see a distended or “bowed” interatrial septum, often sloping up to the right on the view merging with some dilated pulmonary veins. In a volume-overloaded heart, the high pressure in the left atrium often causes the septum to bulge significantly into the right atrium.
Clinical Recommendation: When the septum is distended, do not measure from the most “sunken” point. Instead, measure from the middle of the septal curvature to the posterior wall, ensuring your line remains strictly parallel to the mitral annulus. Subjectively, a septum that loses its horizontal orientation and “blows out” into the right heart is a strong red flag for elevated filling pressures, even if your linear measurement is borderline.
This is never going to be a perfect appraoch. Realistically, if you want a reliable comparative measure of LA size at this point, you would need to measure the LA area. But that’s not yet something I see cardiologists actually doing clinically.
Normalisation: The LADn Calculation
Because the LAD is a linear measurement in centimetres, it is not weight-independent like a ratio. It must be normalised to body weight using an allometric scaling formula to be clinically useful.
Of course, measuring a patient’s weight is much easier and more accurate than measuring the aortic root size reliably, so this generates a lot less error. However, as with any normalised measurement, take care if the patient is very obese or underweight.
The formula for the normalised left atrial diameter (LADn) is:
LADn = LAD (cm) Weight (kg)0.309
But don't try and put it in a standard calculator - use our online tool which you can use as an app on your phone and can support all the many echo measurements, ratios and indicies out there!
Try the VetCardioHub Echo Calculator| Metric | Normal Range | Stage B2 Threshold |
|---|---|---|
| LADn | 1.05 – 1.6 | 1.6 |
Table 1: Clinical thresholds for LADn in dogs.
Adding LAD to EPIC Interpretation
While the original EPIC trial criteria strictly use the short-axis LA:Ao > 1.6, the LADn serves as a powerful “second opinion”.
-
Higher Repeatability: The inter-operator coefficient of variation for LAD is only 2.2%, compared to nearly 7% for LA:Ao. And this is in skilled hands. This makes it much more reliable for serial monitoring of the same dog over time.
-
The Tie-Breaker: If you have a dog with a borderline LA:Ao (e.g., 1.55) but the LADn is clearly enlarged (e.g., 1.65), you should have much higher confidence that the patient is transitioning into Stage B2 and requires intervention.
Note: Many studies have quoted upper limit numbers in the 1.53-1.6 range, for simplicity I use 1.6 in practice. But like in all things its a grey area not an exact cut off, so if you get 1.58 and you have other signs of stage B2 I would probably think thats significant.
The Feline Standard
In cats, the LAD is now considered by most cardiologists to be the primary metric. Due to high feline heart rates, short-axis timing is often a guessing game.


-
Feline Cut-off: An LAD > 16 mm is considered enlarged in most cats. Although some consideration should be made for size of cat, if its sitting in the 'grey zone' which I would class as 17-19mm.
-
Risk Zone: Any cat with an LAD > 20 mm is at high risk for blood stasis and aortic thromboembolism (ATE), and clopidogrel should be discussed with the owner immediately.
Clinical Takeaways
-
Trust the Long Axis: If the short-axis view is giving you an “oval” aorta or inconsistent numbers, switch to the RPLA4Ch view. It is harder to get “off-axis” here.
-
Timing is Everything: Remember that while LA:Ao is an early-diastolic measurement, LAD is end-systolic (the largest atrium).
-
The 1.6 Threshold: Use LADn > 1.6 as your red flag for dogs. If both your LA:Ao and your LADn are up, the case for Stage B2 is ironclad.
-
Monitoring: When monitoring a patient, look at the LAD measurement over time and see what it’s doing. No need to normalise.
-
Obesity: Normalisation assumes a patient is of a standard body fat percentage. If a patient is very over or underweight, this will skew the formula slightly. Obese patients will have a lower normalised number than usual, and underweight patients will be higher. This is also true in skinny breeds, like sighthounds.